
Fillable Printable Vba 29 1546 Are
Fillable Printable Vba 29 1546 Are
Vba 29 1546 Are
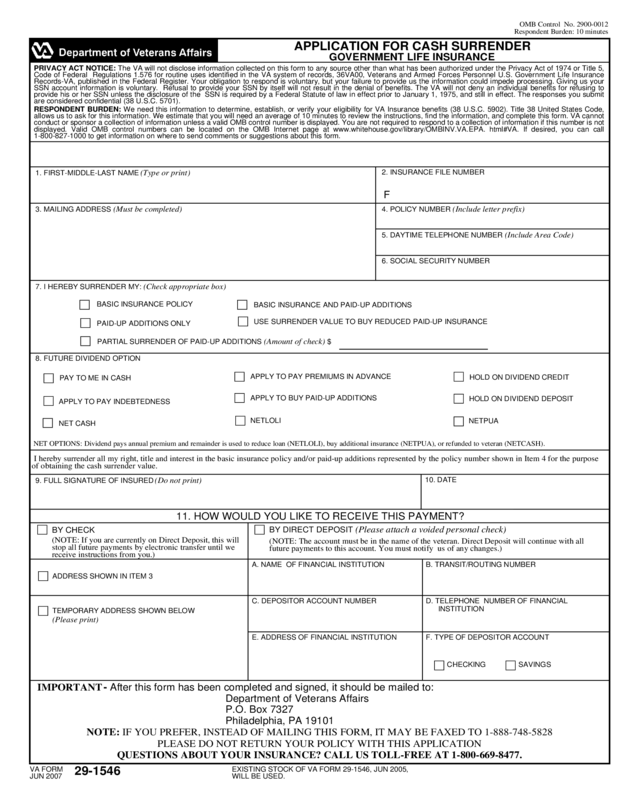
APPLICATION FOR CASH SURRENDER
GOVERNMENT LIFE INSURANCE
OMB Control No. 2900-0012
Respondent Burden: 10 minutes
VA FORM
JUN 2007
29-1546
EXISTING STOCK OF VA FORM 29-1546, JUN 2005,
WILL BE USED.
1. FIRST-MIDDLE-LAST NAME (Type or print)
F
2. INSURANCE FILE NUMBER
NET OPTIONS: Dividend pays annual premium and remainder is used to reduce loan (NETLOLI), buy additional insurance (NETPUA), or refunded to veteran (NETCASH).
10. DATE
11. HOW WOULD YOU LIKE TO RECEIVE THIS PAYMENT?
BY DIRECT DEPOSIT (Please attach a voided personal check)
(NOTE: If you are currently on Direct Deposit, this will
stop all future payments by electronic transfer until we
receive instructions from you.)
ADDRESS SHOWN IN ITEM 3
QUESTIONS ABOUT YOUR INSURANCE? CALL US TOLL-FREE AT 1-800-669-8477.
NOTE: IF YOU PREFER, INSTEAD OF MAILING THIS FORM, IT MAY BE FAXED TO 1-888-748-5828
PLEASE DO NOT RETURN YOUR POLICY WITH THIS APPLICATION
IMPORTANT - After this form has been completed and signed, it should be mailed to:
Department of Veterans Affairs
P.O. Box 7327
Philadelphia, PA 19101
D. TELEPHONE NUMBER OF FINANCIAL
INSTITUTION
SAVINGS
I hereby surrender all my right, title and interest in the basic insurance policy and/or paid-up additions represented by the policy number shown in Item 4 for the purpose
of obtaining the cash surrender value.
4. POLICY NUMBER (Include letter prefix) 3. MAILING ADDRESS (Must be completed)
5. DAYTIME TELEPHONE NUMBER (Include Area Code)
A. NAME OF FINANCIAL INSTITUTION
6. SOCIAL SECURITY NUMBER
8. FUTURE DIVIDEND OPTION
7. I HEREBY SURRENDER MY: (Check appropriate box)
PARTIAL SURRENDER OF PAID-UP ADDITIONS (Amount of check) $
9. FULL SIGNATURE OF INSURED (Do not print)
BY CHECK
(NOTE: The account must be in the name of the veteran. Direct Deposit will continue with all
future payments to this account. You must notify us of any changes.)
E. ADDRESS OF FINANCIAL INSTITUTION F. TYPE OF DEPOSITOR ACCOUNT
B. TRANSIT/ROUTING NUMBER
TEMPORARY ADDRESS SHOWN BELOW
(Please print)
C. DEPOSITOR ACCOUNT NUMBER
BASIC INSURANCE POLICY
BASIC INSURANCE AND PAID-UP ADDITIONS
USE SURRENDER VALUE TO BUY REDUCED PAID-UP INSURANCE
APPLY TO PAY PREMIUMS IN ADVANCE
APPLY TO BUY PAID-UP ADDITIONS
PAID-UP ADDITIONS ONLY
NETLOLI
HOLD ON DIVIDEND CREDIT
HOLD ON DIVIDEND DEPOSIT
NETPUA
PAY TO ME IN CASH
APPLY TO PAY INDEBTEDNESS
NET CASH
CHECKING
PRIVACY ACT NOTICE: The VA will not disclose information collected on this form to any source other than what has been authorized under the Privacy Act of 1974 or Title 5,
Code of Federal Regulations 1.576 for routine uses identified in the VA system of records, 36VA00, Veterans and Armed Forces Personnel U.S. Government Life Insurance
Records-VA, published in the Federal Register. Your obligation to respond is voluntary, but your failure to provide us the information could impede processing. Giving us your
SSN account information is voluntary. Refusal to provide your SSN by itself will not result in the denial of benefits. The VA will not deny an individual benefits for refusing to
provide his or her SSN unless the disclosure of the SSN is required by a Federal Statute of law in effect prior to January 1, 1975, and still in effect. The responses you submit
are considered confidential (38 U.S.C. 5701).
RESPONDENT BURDEN: We need this information to determine, establish, or verify your eligibility for VA Insurance benefits (38 U.S.C. 5902). Title 38 United States Code,
allows us to ask for this information. We estimate that you will need an average of 10 minutes to review the instructions, find the information, and complete this form. VA cannot
conduct or sponsor a collection of information unless a valid OMB control number is displayed. You are not required to respond to a collection of information if this number is not
displayed. Valid OMB control numbers can be located on the OMB Internet page at www.whitehouse.gov/library/OMBINV.VA.EPA. html#VA. If desired, you can call
1-800-827-1000 to get information on where to send comments or suggestions about this form.
APPLICATION FOR POLICY LOAN
GOVERNMENT LIFE INSURANCE
OMB Approved No. 2900-0012
Respondent Burden: 10 minutes
1. FIRST-MIDDLE-LAST NAME (Type or print)
F
IMPORTANT NOTICE
MAXIMUM LOAN
All new policy loans have a variable interest rate with a minimum rate of 5% and a maximum rate of
12%. The interest rate may change October of each year. The rate is based on the interest for long term
Treasury bonds. Interest is payable yearly on the anniversary date of the loan.
10. DATE
11. HOW WOULD YOU LIKE TO RECEIVE THIS PAYMENT?
BY DIRECT DEPOSIT (Please attach a voided personal check)
(NOTE: If you are currently on Direct Deposit, this will
stop all future payments by electronic transfer until we
receive instructions from you.)
ADDRESS SHOWN IN ITEM 3
VA FORM
JUN 2007
29-1546
QUESTIONS ABOUT YOUR INSURANCE? CALL US TOLL-FREE AT 1-800-669-8477.
EXISTING STOCK OF VA FORM 29-1546, JUN 2005,
WILL BE USED.
NOTE: IF YOU PREFER, INSTEAD OF MAILING THIS FORM, IT MAY BE FAXED TO 1-888-748-5828
PLEASE DO NOT RETURN YOUR POLICY WITH THIS APPLICATION
IMPORTANT - After this form has been completed and signed, it should be mailed to:
Department of Veterans Affairs
P.O. Box 7327
Philadelphia, PA 19101
D. TELEPHONE NUMBER OF FINANCIAL
INSTITUTION
SAVINGS
$
APPLY EXISTING DIVIDEND CREDIT/DEPOSIT TO REDUCE THE LOAN
PRINCIPAL
NOTE: Your VA compensation or pension or military retirement pay may be used to repay your loan. For more information, call the toll-free number below.
2. INSURANCE FILE NUMBER
3. MAILING ADDRESS (Must be completed)
5. DAYTIME TELEPHONE NUMBER (Include Area Code)
A. NAME OF FINANCIAL INSTITUTION
7. AMOUNT OF LOAN DESIRED (Check one)
4. SOCIAL SECURITY NUMBER
8. DO YOU WISH TO USE DIVIDENDS TO REDUCE THE LOAN?
6. POLICY NUMBER(S) ON WHICH LOAN IS REQUESTED
APPLY FUTURE DIVIDENDS TO REDUCE LOAN PRINCIPAL
APPLY FUTURE DIVIDENDS TO PAY AN ANNUAL PREMIUM WITH THE
REMAINING BALANCE APPLIED TO REDUCE THE LOAN
9. FULL SIGNATURE OF INSURED (Do not print)
BY CHECK
(NOTE: The account must be in the name of the veteran. Direct Deposit will continue with all
future payments to this account. You must notify us of any changes.)
E. ADDRESS OF FINANCIAL INSTITUTION F. TYPE OF DEPOSITOR ACCOUNT
B. TRANSIT/ROUTING NUMBER
TEMPORARY ADDRESS SHOWN BELOW
(Please print)
C. DEPOSITOR ACCOUNT NUMBER
CHECKING
(AMOUNT) OR
RESPONDENT BURDEN: We need this information to determine, establish, or verify your eligibility for VA Insurance benefits (38 U.S.C. 5902). Title 38 United States Code,
allows us to ask for this information. We estimate that you will need an average of 10 minutes to review the instructions, find the information, and complete this form. VA cannot
conduct or sponsor a collection of information unless a valid OMB control number is displayed. You are not required to respond to a collection of information if this number is not
displayed. Valid OMB control numbers can be located on the OMB Internet page at www.whitehouse.gov/library/OMBINV.VA.EPA. html#VA. If desired, you can call
1-800-827-1000 to get information on where to send comments or suggestions about this form.
PRIVACY ACT NOTICE: The VA will not disclose information collected on this form to any source other than what has been authorized under the Privacy Act of 1974 or Title 5,
Code of Federal Regulations 1.576 for routine uses identified in the VA system of records, 36VA00, Veterans and Armed Forces Personnel U.S. Government Life Insurance
Records-VA, published in the Federal Register. Your obligation to respond is voluntary, but your failure to provide us the information could impede processing. Giving us your
SSN account information is voluntary. Refusal to provide your SSN by itself will not result in the denial of benefits. The VA will not deny an individual benefits for refusing to
provide his or her SSN unless the disclosure of the SSN is required by a Federal Statute of law in effect prior to January 1, 1975, and still in effect. The responses you submit
are considered confidential (38 U.S.C. 5701).


