
- Form FS-48 - Financial Security Exemption Application - New York
- Form FS-113 - Certificate of Removal from US and Canada - New York
- Form MV-994 - Bond Under the State Vehicle and Traffic Law - New York
- Form FM-11 - 2014 Premiums for Assessment Statement - New York
- Form MV-197 - Exempt Vehicle Certificate - New York
Fillable Printable Form FM-11 - 2014 Premiums for Assessment Statement - New York
Fillable Printable Form FM-11 - 2014 Premiums for Assessment Statement - New York
Form FM-11 - 2014 Premiums for Assessment Statement - New York
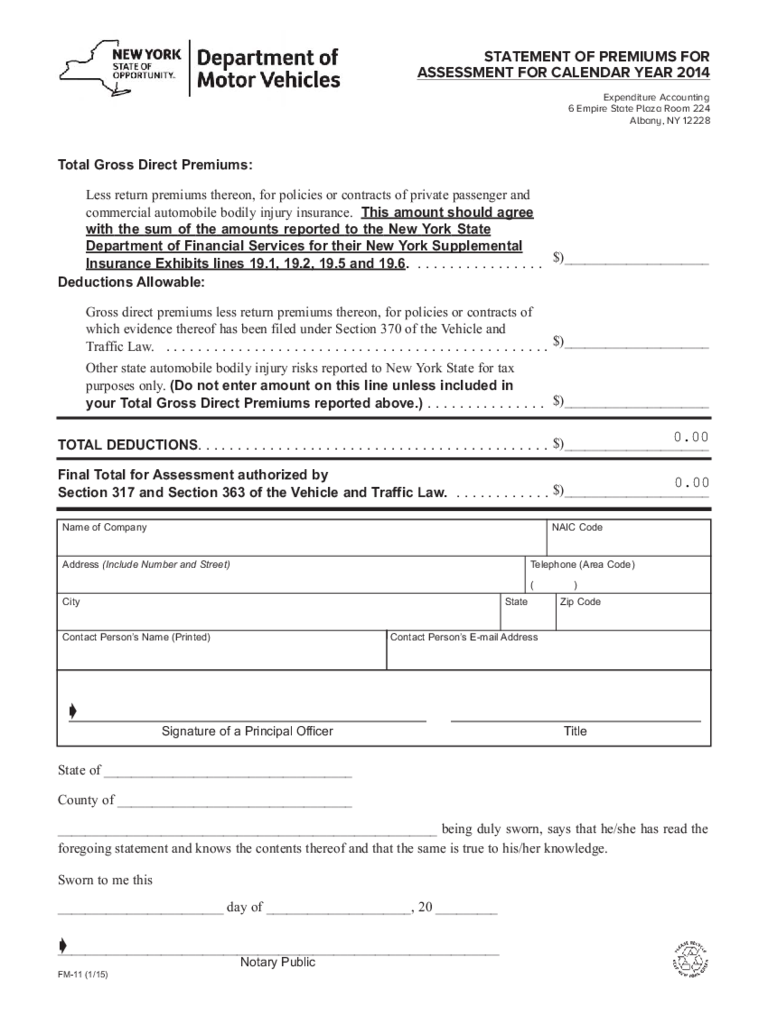
STATEMENT OF PREMIUMS FOR
ASSESSMENT FOR CALENDAR YEAR 2014
Expenditure Accounting
6 Empire State Plaza Room 224
Albany, NY 12228
Total Gross Direct Premiums:
Less return premiums thereon, for policies or contracts of private passenger and
commercial automobile bodily injury insurance. This amount should agree
with the sum of the amounts reported to the New York State
Department of Financial Services for their New York Supplemental
Insurance Exhibits lines 19.1, 19.2, 19.5 and 19.6. . . . . . . . . . . . . . . . .
Deductions Allowable:
Gross direct premiums less return premiums thereon, for policies or contracts of
which evidence thereof has been filed under Section 370 of the Vehicle and
Traffic Law. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
State of ____________________________________
County of __________________________________
_______________________________________________________ being duly sworn, says that he/she has read the
foregoing statement and knows the contents thereof and that the same is true to his/her knowledge.
Sworn to me this
________________________ day of _____________________, 20 _________
________________________________________________________________
TOTAL DEDUCTIONS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Other state automobile bodily injury risks reported to New York State for tax
purposes only. (Do not enter amount on this line unless included in
your Total Gross Direct Premiums reported above.) . . . . . . . . . . . . . . .
Final Total for Assessment authorized by
Section 317 and Section 363 of the Vehicle and Traffic Law. . . . . . . . . . . . .
FM-11 (1/15)
$)_____________________
$)_____________________
$)_____________________
$)_____________________
$)_____________________
Name of Company
Address (Include Number and Street) Telephone (Area Code)
( )
City
ç
ç
Signature of a Principal Officer
Notary Public
Title
State Zip Code
NAIC Code
Contact Person’s Name (Printed) Contact Person’s E-mail Address
0.00
0.00
reset/clear


