
- Form MV-262 - Certification of Supervised Driving - New York
- Form MV-TEENS - TEENS Enrollment and Consent Form - New York
- Form MV-619 - Vision Test Report - New York
- Form ID-44EDL - Proofs of Identity, U.S. Citizenship and Residency - New York
- Form MV-58A - Certificate of Employment - New York
- Form MV-80W - Application for Tinted Window Exemption - New York
Fillable Printable Form MV-80 - Physician's Statement - New York
Fillable Printable Form MV-80 - Physician's Statement - New York
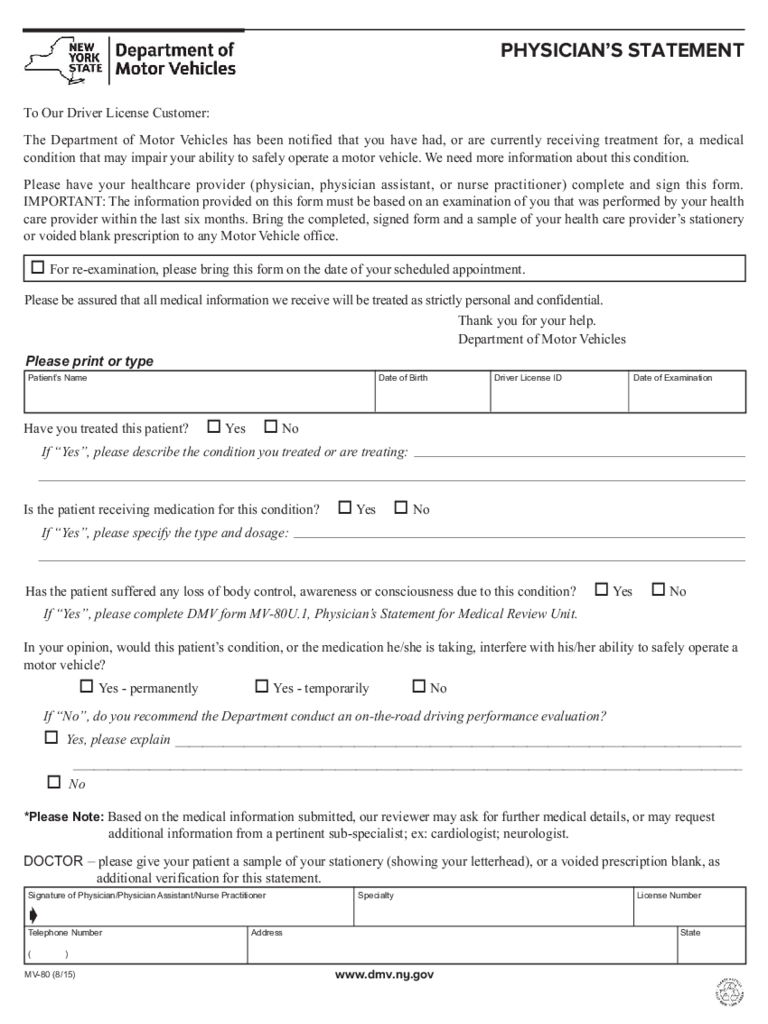
Form MV-80 - Physician's Statement - New York
www.dmv.ny.gov
To Our Driver License Customer:
The Department of Motor Vehicles has been notified that you have had, or are currently receiving treatment for, a medical
condition that may impair your ability to safely operate a motor vehicle. We need more information about this condition.
Please have your healthcare provider (physician, physician assistant, or nurse practitioner) complete and sign this form.
IMPORTANT: The information provided on this form must be based on an examination of you that was performed by your health
care provider within the last six months. Bring the completed, signed form and a sample of your health care provider’s stationery
or voided blank prescription to any Motor Vehicle office.
o For re-examination, please bring this form on the date of your scheduled appointment.
Please be assured that all medical information we receive will be treated as strictly personal and confidential.
Thank you for your help.
Department of Motor Vehicles
PHYSICIAN’S STATEMENT
Patient’s Name Date of Birth Date of Examination
Please print or type
Signature of Physician/Physician Assistant/Nurse Practitioner
Telephone Number
( )
Address
Specialty License Number
State
Have you treated this patient? o Yes o No
If “Yes”, please describe the condition you treated or are treating:
If “No”, do you recommend the Department conduct an on-the-road driving performance evaluation?
o Yes, please explain __________________________________________________________________________________
_________________________________________________________________________________________________
o No
In your opinion, would this patient’s condition, or the medication he/she is taking, interfere with his/her ability to safely operate a
motor vehicle?
o Yes - permanently o Yes - temporarily o No
Has the patient suffered any loss of body control, awareness or consciousness due to this condition? o Yes o No
If “Yes”, please complete DMV form MV-80U.1, Physician’s Statement for Medical Review Unit.
Is the patient receiving medication for this condition? o Yes o No
If “Yes”, please specify the type and dosage:
DOCTOR – please give your patient a sample of your stationery (showing your letterhead), or a voided prescription blank, as
additional verification for this statement.
MV-80 (8/15)
ç
Driver License ID
*Please Note: Based on the medical information submitted, our reviewer may ask for further medical details, or may request
additional information from a pertinent sub-specialist; ex: cardiologist; neurologist.


