
Fillable Printable Sample Child Coordination of Benefits Form
Fillable Printable Sample Child Coordination of Benefits Form
Sample Child Coordination of Benefits Form
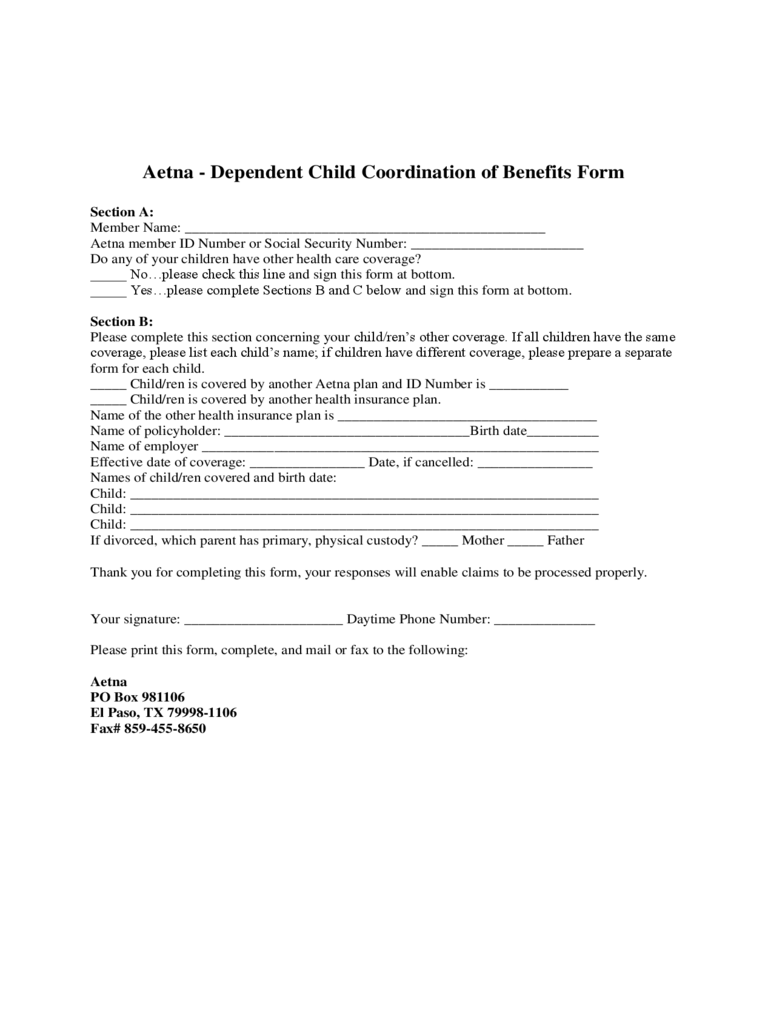
Aetna - Dependent Child Coordination of Benefits Form
Section A:
Member Name: __________________________________________________
Aetna member ID Number or Social Security Number: ________________________
Do any of your children have other health care coverage?
_____ No…please check this line and sign this form at bottom.
_____ Yes…please complete Sections B and C below and sign this form at bottom.
Section B:
Please complete this section concerning your child/ren’s other coverage. If all children have the same
coverage, please list each child’s name; if children have different coverage, please prepare a separate
form for each child.
_____ Child/ren is covered by another Aetna plan and ID Number is ___________
_____ Child/ren is covered by another health insurance plan.
Name of the other health insurance plan is ____________________________________
Name of policyholder: __________________________________Birth date__________
Name of employer _______________________________________________________
Effective date of coverage: ________________ Date, if cancelled: ________________
Names of child/ren covered and birth date:
Child: _________________________________________________________________
Child: _________________________________________________________________
Child: _________________________________________________________________
If divorced, which parent has primary, physical custody? _____ Mother _____ Father
Thank you for completing this form, your responses will enable claims to be processed properly.
Your signature: ______________________ Daytime Phone Number: ______________
Please print this form, complete, and mail or fax to the following:
Aetna
PO Box 981106
El Paso, TX 79998-1106
Fax# 859-455-8650


