
Fillable Printable Sample Provider Service Invoice Template
Fillable Printable Sample Provider Service Invoice Template
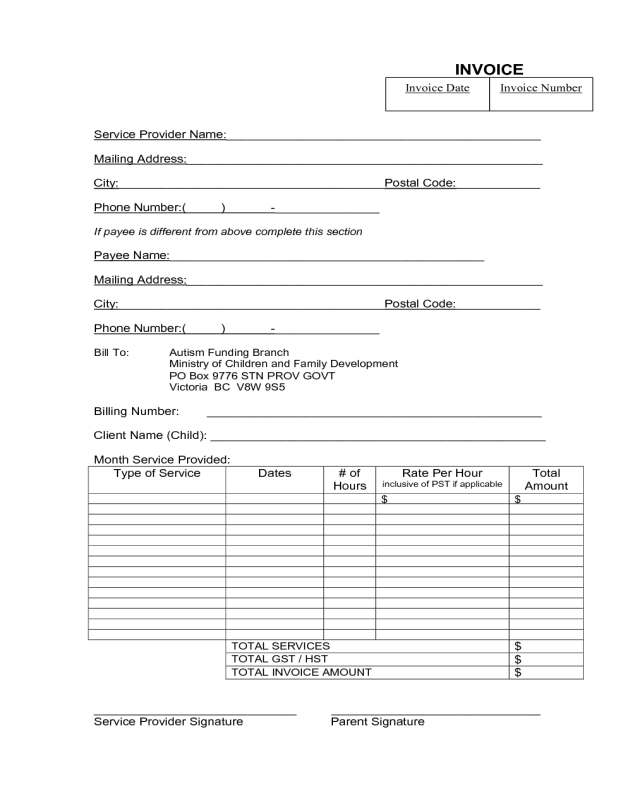
Sample Provider Service Invoice Template
INVOICE
Service Provider Name:_____________________________________________
Mailing Address:___________________________________________________
City:______________________________________Postal Code:____________
Phone Number:( ) -_______________
If payee is different from above complete this section
Payee Name:_____________________________________________
Mailing Address:___________________________________________________
City:______________________________________Postal Code:____________
Phone Number:( ) -_______________
Bill T o : Autism Funding Branch
Ministry of Children and Family Development
PO Box 9776 ST N PROV GOVT
Vict oria BC V8W 9S5
Billing Number: ________________________________________________
Clien t Name (Child): ________________________________________________
Month Service Provided:
Type of Service
Dates
# of
Hours
Rate Per Hour
inclusive of PST i f applicable
Total
Amount
$
$
TOTAL SERVICES
$
TOTAL GST / HST
$
TOTAL INVOICE AMOUNT
$
_____________________________ ______________________________
Service Provider Signature Parent Signature
Invoice Number
Invoice Date


