
Fillable Printable Worker's Report of Injury - Arizona
Fillable Printable Worker's Report of Injury - Arizona
Worker's Report of Injury - Arizona
THE INDUSTRIAL COMMISSION COMPLIES WITH THE AMERICANS WITH DISABILITIES ACT OF 1990. IF YOU NEED THIS DOCUMENT IN ALTERNATIVE FORMAT, CONTACT CLAIMS AT (602 542-4661).
ICA 04-0407 REV 5/02
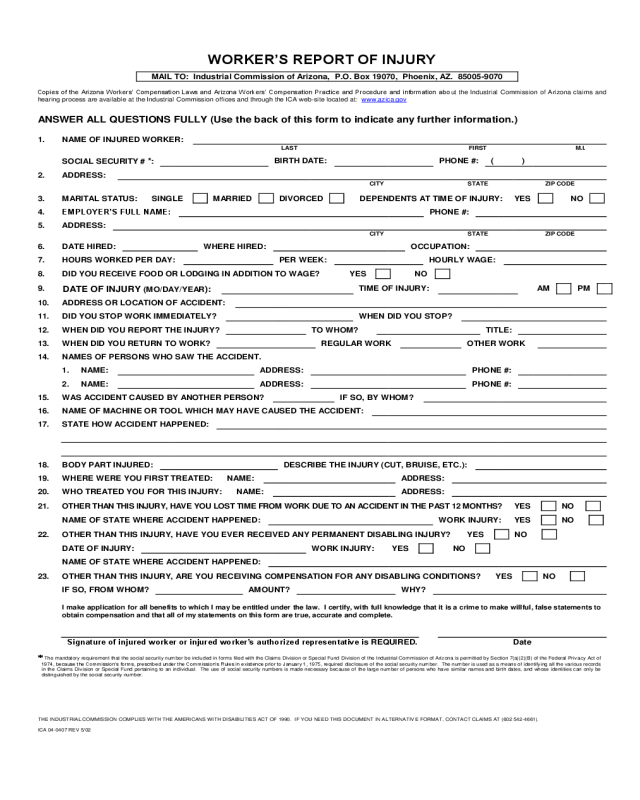
WORKER’S REPORT OF INJURY
MAIL TO: Industrial Commission of Arizona, P.O. Box 19070, Phoenix, AZ. 85005-9070
Copies of the Arizona Workers’ Compensation Laws and Arizona Workers’ Compensation Practice and Procedure and information about the Industrial Commission of Arizona claims and
hearing process are available at the Industrial Commission offices and through the ICA web-site located at: www.azica.gov
ANSWER ALL QUESTIONS FULLY (Use the back of this form to indicate any further information.)
1.
NAME OF INJURED WORKER:
LAST
FIRST
M.I.
SOCIAL SECURITY # *:
BIRTH DATE:
PHONE #:
( )
2.
ADDRESS:
CITY
STATE
ZIP CODE
3.
MARITAL STATUS:
SINGLE
MARRIED
DIVORCED
DEPENDENTS AT TIME OF INJURY:
YES
NO
4.
EMPLOYER’S FULL NAME:
PHONE #:
5.
ADDRESS:
CITY
STATE
ZIP CODE
6.
DATE HIRED:
WHERE HIRED:
OCCUPATION:
7.
HOURS WORKED PER DAY:
PER WEEK:
HOURLY WAGE:
8.
DID YOU RECEIVE FOOD OR LODGING IN ADDITION TO WAGE?
YES
NO
9.
DATE OF INJURY (MO/DAY/YEAR):
TIME OF INJURY:
AM
PM
10.
ADDRESS OR LOCATION OF ACCIDENT:
11.
DID YOU STOP WORK IMMEDIATELY?
WHEN DID YOU STOP?
12.
WHEN DID YOU REPORT THE INJURY?
TO WHOM?
TITLE:
13.
WHEN DID YOU RETURN TO WORK?
REGULAR WORK
OTHER WORK
14.
NAMES OF PERSONS WHO SAW THE ACCIDENT.
1.
NAME:
ADDRESS:
PHONE #:
2.
NAME:
ADDRESS:
PHONE #:
15.
WAS ACCIDENT CAUSED BY ANOTHER PERSON?
IF SO, BY WHOM?
16.
NAME OF MACHINE OR TOOL WHICH MAY HAVE CAUSED THE ACCIDENT:
17.
STATE HOW ACCIDENT HAPPENED:
18.
BODY PART INJURED:
DESCRIBE THE INJURY (CUT, BRUISE, ETC.):
19.
WHERE WERE YOU FIRST TREATED:
NAME:
ADDRESS:
20.
WHO TREATED YOU FOR THIS INJURY:
NAME:
ADDRESS:
21.
OTHER THAN THIS INJURY, HAVE YOU LOST TIME FROM WORK DUE TO AN ACCIDENT IN THE PAST 12 MONTHS?
YES
NO
NAME OF STATE WHERE ACCIDENT HAPPENED:
WORK INJURY:
YES
NO
22.
OTHER THAN THIS INJURY, HAVE YOU EVER RECEIVED ANY PERMANENT DISABLING INJURY?
YES
NO
DATE OF INJURY:
WORK INJURY:
YES
NO
NAME OF STATE WHERE ACCIDENT HAPPENED:
23.
OTHER THAN THIS INJURY, ARE YOU RECEIVING COMPENSATION FOR ANY DISABLING CONDITIONS?
YES
NO
IF SO, FROM WHOM?
AMOUNT?
WHY?
I make application for all benefits to which I may be entitled under the law. I certify, with full knowledge that it is a crime to make willful, false statements to
obtain compensation and that all of my statements on this form are true, accurate and complete.
Signature of injured worker or injured worker’s authorized representative is REQUIRED.
Date
The mandatory requirement that the social security number be included in forms filed with the Claims Division or Special Fund Division of the Industrial Commission of Arizona is permitted by Section 7(a)(2)(B) of the Federal Privacy Act of
1974, because the Commission’s forms, prescribed under the Commission’s Rules in existence prior to January 1, 1975, required disclosure of the social security number. The number is used as a means of identifying all the various records
in the Claims Division or Special Fund pertaining to an individual. The use of social security numbers is made necessary because of the large number of persons who have similar names and birth dates, and whose identities can only be
distinguished by the social security number.


