
- Form MV-104D - Police Report for Fatal Motor Vehicle Accidents - New York
- Form MV-104L - Motor Vehicle/Police Line of Duty Accident Report - New York
- Form MV-104F - Accident Report for School Vehicles - New York
- Form MV-198C - Request for Copy of Accident Report - New York
- Form MV-104S - Truck and Bus Supplemental Police Accident Report - New York
- Form MV-104F.1 - Accident Report for School Vehicles - New York
Fillable Printable Form MV-104D - Police Report for Fatal Motor Vehicle Accidents - New York
Fillable Printable Form MV-104D - Police Report for Fatal Motor Vehicle Accidents - New York
Form MV-104D - Police Report for Fatal Motor Vehicle Accidents - New York
Work Related
oYes oNo
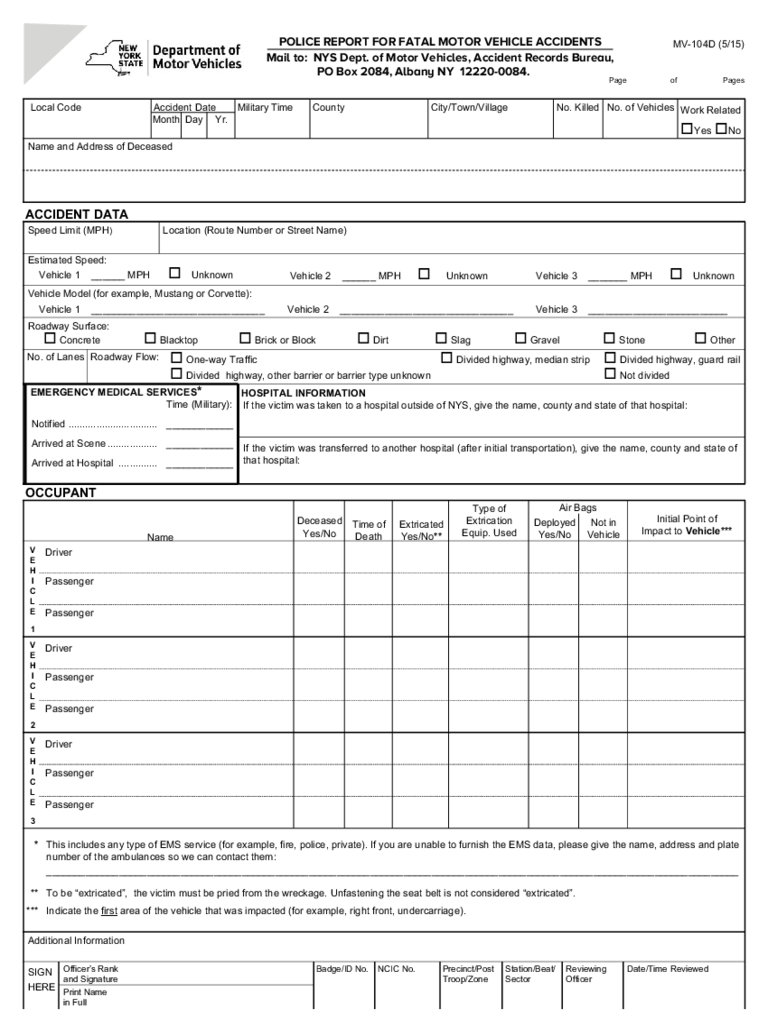
POLICE REPORT FOR FATAL MOTOR VEHICLE ACCIDENTS
Mail to: NYS Dept. of Motor Vehicles, Accident Records Bureau,
PO Box 2084, Albany NY 12220-0084.
Accident Date
Month Day Yr.
Military Time
County
No. of Vehicles
No. KilledCity/Town/Village
No. of Lanes
ACCIDENT DATA
Speed Limit (MPH)
Estimated Speed:
Vehicle Model (for example, Mustang or Corvette):
Roadway Surface:
Roadway Flow:
EMERGENCY MEDICAL SERVICES
*
HOSPITAL INFORMATION
If the victim was transferred to another hospital (after initial transportation), give the name, county and state of
that hospital:
If the victim was taken to a hospital outside of NYS, give the name, county and state of that hospital:
Notified ................................ ____________
Arrived at Scene .................. ____________
Arrived at Hospital .............. ____________
Time (Military):
Vehicle 1 ______ MPH
o Unknown
Vehicle 1 _______________________________
o Concrete o Blacktop o Brick or Block o Dirt o Slag o Gravel o Stone o Other
o One-way Traffic
o Divided highway, other barrier or barrier type unknown
o Divided highway, median strip o Divided highway, guard rail
o Not divided
Vehicle 2 _______________________________ Vehicle 3 _________________________
Vehicle 2 ______ MPH o Unknown Vehicle 3 _______ MPH o Unknown
Location (Route Number or Street Name)
Page of Pages
Local Code
Name and Address of Deceased
OCCUPANT
Name
Driver
Passenger
Passenger
V
E
H
I
C
L
E
1
Driver
Passenger
Passenger
V
E
H
I
C
L
E
2
Driver
Passenger
Passenger
Additional Information
SIGN
HERE
Badge/ID No.Officer’s Rank
and Signature
Print Name
in Full
NCIC No. Precinct/Post
Troop/Zone
Station/Beat/
Sector
Reviewing
Officer
Date/Time Reviewed
V
E
H
I
C
L
E
3
Deceased
Yes/No
Time of
Death
Extricated
Yes/No**
Initial Point of
Impact to Vehicle***
Type of
Extrication
Equip. Used
Air Bags
Deployed
Yes/No
Not in
Vehicle
* This includes any type of EMS service (for example, fire, police, private). If you are unable to furnish the EMS data, please give the name, address and plate
number of the ambulances so we can contact them:
____________________________________________________________________________________________________________________________
** To be “extricated”, the victim must be pried from the wreckage. Unfastening the seat belt is not considered “extricated”.
*** Indicate the first
area of the vehicle that was impacted (for example, right front, undercarriage).
MV-104D (5/15)


