
- Form MV-104F - Accident Report for School Vehicles - New York
- Form MV-104L - Motor Vehicle/Police Line of Duty Accident Report - New York
- Form MV-104F.1 - Accident Report for School Vehicles - New York
- Form MV-198C - Request for Copy of Accident Report - New York
- Form MV-104S - Truck and Bus Supplemental Police Accident Report - New York
- Form MV-104D - Police Report for Fatal Motor Vehicle Accidents - New York
Fillable Printable Form MV-198C - Request for Copy of Accident Report - New York
Fillable Printable Form MV-198C - Request for Copy of Accident Report - New York
Form MV-198C - Request for Copy of Accident Report - New York
DMV account number
Check/Money Order - Payable to Commissioner of Motor Vehicles
Exempt
Optional - Your reference number:
_________________________________________
Print name and address where the accident report(s) should be mailed:
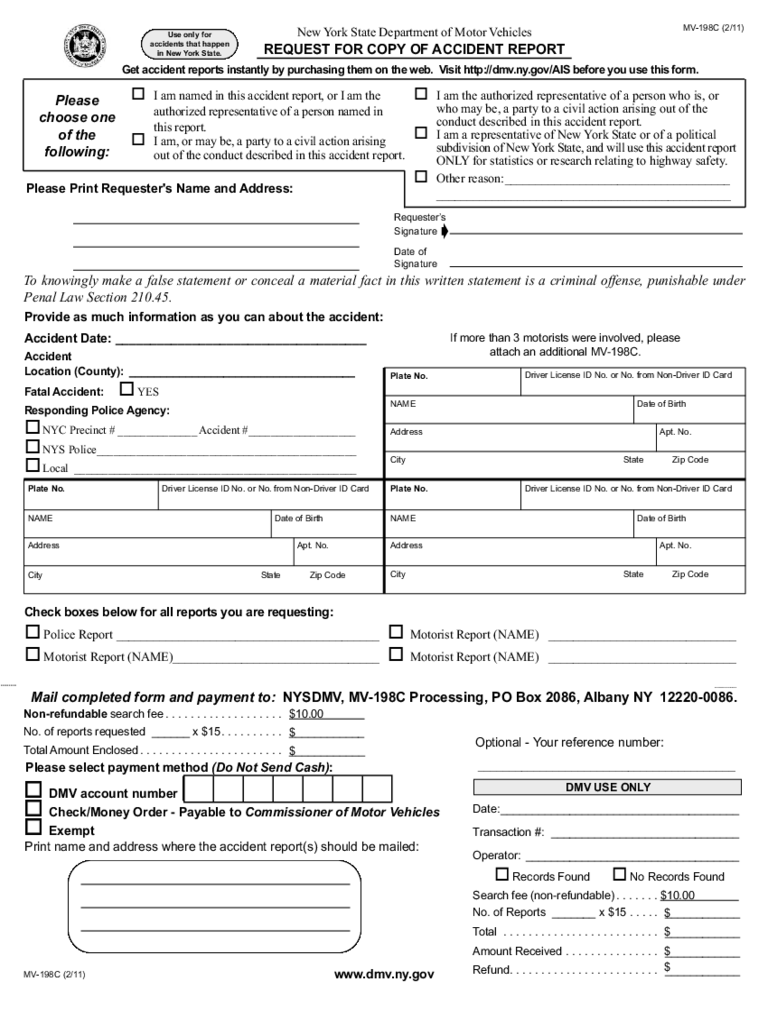
Please select payment method (Do Not Send Cash):
Date:______________________________________
Transaction #: ______________________________
Operator: __________________________________
Records Found No Records Found
Search fee (non-refundable) . . . . . . . $10.00
No. of Reports _______ x $15 . . . . . ____________
Total . . . . . . . . . . . . . . . . . . . . . . . . . ____________
Amount Received . . . . . . . . . . . . . . . ____________
Refund. . . . . . . . . . . . . . . . . . . . . . . . ____________
Non-refundable search fee . . . . . . . . . . . . . . . . . . . $10.00
No. of reports requested ______ x $15 . . . . . . . . . . ____________
Total Amount Enclosed . . . . . . . . . . . . . . . . . . . . . . . ____________
DMV USE ONLY
Apt. No.
NAME
Driver License ID No. or No. from Non-Driver ID Card
Date of Birth
Address
City State Zip Code
Plate No.
To knowingly make a false statement or conceal a material fact in this written statement is a criminal offense, punishable under
Penal Law Section 210.45.
New York State Department of Motor Vehicles
REQUEST FOR COPY OF ACCIDENT REPORT
Requester’s
Signature
Date of
Signature
Apt. No.
NAME
Driver License ID No. or No. from Non-Driver ID Card
Date of Birth
Address
City State Zip Code
Plate No.
Apt. No.
NAME
Driver License ID No. or No. from Non-Driver ID Card
Date of Birth
Address
City State Zip Code
Plate No.
MV-198C (2/11)
MV-198C (2/11)
Please Print Requester's Name and Address:
Check boxes below for all reports you are requesting:
Police Report __________________________________________ Motorist Report (NAME) ______________________________
Motorist Report (NAME)_________________________________ Motorist Report (NAME) ______________________________
Accident Date: ____________________________________
Accident
Location (County): ____________________________________
Fatal Accident:
YES
Responding Police Agency:
NYC Precinct # ______________ Accident #___________________
NYS Police______________________________________________
Local __________________________________________________
±
$
$
$
$
$
$
Provide as much information as you can about the accident:
If more than 3 motorists were involved, please
attach an additional MV-198C.
Mail completed form and payment to: NYSDMV, MV-198C Processing, PO Box 2086, Albany NY 12220-0086.
www.dmv.ny.gov
Please
choose one
of the
following:
I am named in this accident report, or I am the
authorized representative of a person named in
this report.
I am, or may be, a party to a civil action arising
out of the conduct described in this accident report.
I am the authorized representative of a person who is, or
who may be, a party to a civil action arising out of the
conduct described in this accident report.
I am a representative of New York State or of a political
subdivision of New York State, and will use this accident report
ONLY for statistics or research relating to highway safety.
Other reason:____________________________________
_______________________________________________
Use only for
accidents that happen
in New York State.
Get accident reports instantly by purchasing them on the web. Visit http://dmv.ny.gov/AIS before you use this form.
reset/clear


