
Fillable Printable Income Statement Form - Nebraska
Fillable Printable Income Statement Form - Nebraska
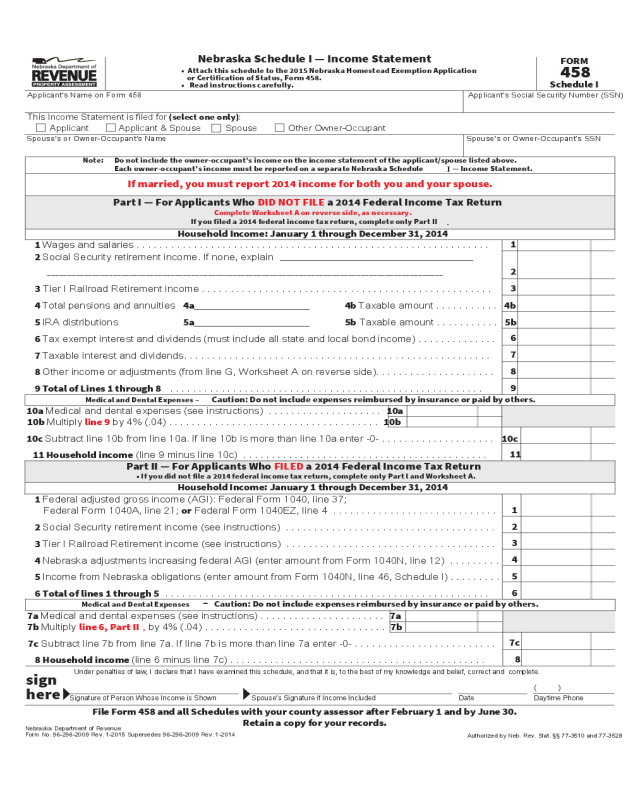
Income Statement Form - Nebraska
This Income Statement is filed for (select one only):
Applicant Applicant & Spouse Spouse Other Owner-Occupant
Applicant’s Name on Form 458 Applicant’s Social Security Number (SSN)
458
Schedule I
FORM
Nebraska Department of Revenue
Form No. 96-296-2009 Rev. 1-2015 Supersedes 96-296-2009 Rev. 1-2014
Authorized by Neb. Rev. Stat. §§ 77-3510 and 77-3528
Part I — For Applicants Who DID NOT FILE a 2014 Federal Income Tax Return
Complete Worksheet A on reverse side, as necessary.
If you filed a 2014 federal income tax return, complete only Part II
.
If married, you must report 2014 income for both you and your spouse.
Household Income: January 1 through December 31, 2014
Part II — For Applicants Who FILED a 2014 Federal Income Tax Return
• If you did not file a 2014 federal income tax return, complete only Part I and Worksheet A.
Household Income: January 1 through December 31, 2014
Signature of Person Whose Income is Shown Spouse’s Signature if Income Included Date Daytime Phone
( )
Under penalties of law, I declare that I have examined this schedule, and that it is, to the best of my knowledge and belief, correct and complete.
Nebraska Schedule I — Income Statement
File Form 458 and all Schedules with your county assessor after February 1 and by June 30.
Retain a copy for your records.
• Attach this schedule to the 2015 Nebraska Homestead Exemption Application
or Certification of Status, Form 458.
• Read instructions carefully.
Note: Do not include the owner-occupant’s income on the income statement of the applicant/spouse listed above.
Each owner-occupant’s income must be reported on a separate Nebraska Schedule
I
— Income Statement.
sign
here
Spouse’s or Owner-Occupant’s Name Spouse’s or Owner-Occupant’s SSN
1 Federal adjusted gross income (AGI): Federal Form 1040, line 37;
Federal Form 1040A, line 21; or Federal Form 1040EZ, line 4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1
2 Social Security retirement income (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2
3 Tier I Railroad Retirement income (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3
4 Nebraska adjustments increasing federal AGI (enter amount from Form 1040N, line 12) . . . . . . . . .
4
5 Income from Nebraska obligations (enter amount from Form 1040N, line 46, Schedule I) . . . . . . . . .
5
6 Total of lines 1 through 5 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6
7a Medical and dental expenses (see instructions) . . . . . . . . . . . . . . . . . . . . . . 7a
7b Multiply line 6, Part II
,
by 4% (.04) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7b
7c Subtract line 7b from line 7a. If line 7b is more than line 7a enter -0- . . . . . . . . . . . . . . . . . . . . . . . . .
7c
8 Household income (line 6 minus line 7c) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8
1 Wages and salaries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1
2 Social Security retirement income. If none, explain
______________________________________________
________________________________________________________________________________________________
2
3 Tier I Railroad Retirement income . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3
4 Total pensions and annuities 4a______________________ 4b Taxable amount . . . . . . . . . . . 4b
5 IRA distributions 5a______________________ 5b Taxable amount . . . . . . . . . . . 5b
6 Tax exempt interest and dividends (must include all state and local bond income) . . . . . . . . . . . . . .
6
7 Taxable interest and dividends. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7
8 Other income or adjustments (from line G, Worksheet A on reverse side). . . . . . . . . . . . . . . . . . . . .
8
9 Total of Lines 1 through 8 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
9
10a Medical and dental expenses (see instructions) . . . . . . . . . . . . . . . . . . . . 10a
10b Multiply line 9 by 4% (.04) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10b
10c Subtract line 10b from line 10a. If line 10b is more than line 10a enter -0- . . . . . . . . . . . . . . . . . . . . 10c
11 Household income (line 9 minus line 10c) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11
Medical and Dental Expenses – Caution: Do not include expenses reimbursed by insurance or paid by others.
Medical and Dental Expenses
–
Caution: Do not include expenses reimbursed by insurance or paid by others.
A Net business income including rental, or farm income, or (loss) .........................................................
A
B Capital gain or (loss) ...........................................................................................................................
B
C Other gain or (loss) .............................................................................................................................
C
D Unemployment compensation .............................................................................................................
D
E Any other income or (adjustments reducing income.) Explain:
E
F Penalty on early withdrawal of savings................................................................................................
F
G Total of lines A through E, minus line F (enter this amount here and on Part I, line 8) ...................
G
Worksheet A — Part I
Line 8, Other Income or Adjustments
Retain a copy for your records.
FORM 458
Schedule I
Worksheet A
Instructions
Who Must File.
This Form 458 Schedule I must be filed by persons applying for a homestead exemption, who are not filing
as a veteran drawing compensation from the Department of Veteran’s Affairs (DVA) or as a paraplegic veteran or multiple
amputee whose home was substantially contributed to by the DVA. This form is to be attached to and filed with the Nebraska
Homestead Exemption Application or Certification of Status, Form 458. (See Form 458 Instructions). If you filed, or would
have filed as married for Nebraska individual income tax purposes for 2014, you must include income for both you and your
spouse, even if you filed as “married, filing separately.” Each additional owner who occupied the homestead during any part
of 2014 must also report their income on a separate schedule.
When and Where to File.
Schedule I must be attached to the Form 458 and filed with your county assessor, after
February 1, 2015 and by June 30, 2015.
Specific Instructions
Note –
Do NOT include the following on the income statement:
• Department of Veterans Affairs disability compensation;
• Supplemental Security Income (SSI);
• Worker’s Compensation Act payments;
• Child support payments;
• Aid to Dependent Children (ADC); and
• Nebraska Department of Health and Human Services aid.
Exclude Social Security payments based on disability for applicants and spouses under their full retirement age (generally
age 66) EXCEPT for any portion of the benefits included in federal adjusted gross income (AGI). Disability benefits
automatically convert to retirement benefits at full retirement age and must be reported. See SSA Publication No. 05-10035.
Part
I
Line 1, Wages and Salaries.
Include any wages, salaries, fees, commissions, tips, bonuses, etc. received in 2014, even
if you do not have a Federal Form W-2. If you have a Federal Form W-2, this information is shown in Box 1.
Line 2, Social Security Retirement Income.
Report net benefits received in 2014, as shown in Box 5, Federal
Form SSA-1099. Do NOT subtract Medicare premiums or any other adjustments from the amount in Box 5.
Line 3, Tier I
Railroad Retirement Income.
Include Tier I net Social Security equivalent benefit received in 2014, as
shown in Box 5, Federal Form RRB-1099.
Line 4a and 4b, Total Pensions and Annuities.
On line 4a, include total payments from retirement plans, life insurance
annuity contracts, profit-sharing plans, and employee savings plans. Include any gross distribution received in 2014, as shown
in Box 1, Federal Form 1099-R. Include Tier II, contributory amount paid, vested dual benefits, and supplemental annuities
as shown in Box 7, Federal Form RRB-1099-R. On line 4b, report the taxable amount from Box 2(a), Form 1099-R. See
Federal Form 1099-R and IRS Publication 575.
Line 5a and 5b, IRA Distributions.
On line 5a, report the total payments received in 2014 from your IRA as shown in
Box 1, Federal Form 1099-R. On line 5b, report the taxable amount from Box 2(a), Form 1099-R. Do not report any amount
from a qualified IRA rollover. See Federal Form 1099-R and IRS Publication 590.
Line 6, Tax Exempt Interest and Dividends.
Report the total interest received in 2014 on tax exempt obligations. State
and local bond income from both Nebraska and out-of-state obligations must be included. Include any exempt interest from
a mutual fund or other regulated investment company. Do not include interest earned on your IRA, or excludable interest on
series EE bonds. See Federal Form 8815.

Line 7, Taxable Interest and Dividends.
Include your total interest and dividends received in 2014, as shown in:
1. Box 1 and Box 3, Federal Form 1099-INT (Interest Income) or similar statement;
2. Box 1 and Box 2, Federal Form 1099-OID; and
3. Box 1a and Box 2a, Federal Form 1099-DIV.
Interest and dividends from all U.S. government obligations must be included.
Line 8, Other Income or Adjustments.
Complete Worksheet A and enter the amount from line G.
Line 9, Total of Lines 1 Through 8.
If the amount on line 9 qualifies you for 100% relief (see the Household Income
Table in these instructions), it is not necessary to complete line 10. In this case, the line 9 amount may be entered on line 11.
Line 10a-10c, Medical and Dental Expenses.
See medical expenses specific instructions on next page.
Line 11. Household Income.
Use this amount to determine your percentage of relief as found in the Household Income
Table in these instructions.
Part II
Line 1, Federal AGI.
Include income as reported for federal income tax purposes on line 37, Federal Form 1040; line 21,
Federal Form 1040A; or line 4, Federal Form 1040EZ.
Line 2, Social Security Retirement Income.
Enter Social Security retirement benefits minus any portion included
as taxable in AGI. This is the amount shown in Box 5, Federal Form SSA-1099 (line 20a, Federal Form 1040, or line 14a,
Federal Form 1040A), minus any amount reported on line 20b, Federal Form 1040, or line 14b, Federal Form 1040A. Do
NOT subtract Medicare premiums or any other adjustments from the amount in Box 5.
Line 3, Tier I Railroad Retirement Income.
Include the net Social Security equivalent portion of Tier I benefits minus
any portion included as taxable in AGI. This is the amount shown in Box 5, Federal Form RRB-1099 (line 20a, Federal
Form 1040, or line 14a, Federal Form 1040A), minus any amount reported on line 20b, Federal Form 1040, or line 14b,
Federal Form 1040A.
Line 4, Nebraska Adjustments Increasing federal AGI.
Report the total amount of Nebraska adjustments increasing
federal AGI as shown on line 12, Nebraska Form 1040N. If there is an amount being deducted as a Nebraska net operating
loss carryforward on line 13 of the Form 1040N, subtract the amount on line 13 from the amount on line 12. The difference
must be entered on line 4 of this form, unless the total is a negative amount; then please enter -0-.
Line 5, Income From Nebraska Obligations.
Include the total amount of interest income from Nebraska obligations
as shown on line 46, Schedule I, Nebraska Form 1040N.
Line 6, Total of Lines 1 Through 5.
If the amount on line 6 qualifies you for 100% relief (see the Household Income
Table in these instructions), it is not necessary to complete line 7. In this case, the line 6 amount may be entered on line 8.
Line 7a-7c, Medical and Dental Expenses.
See medical expenses instructions below.
Line 8. Household Income.
Use this amount to determine your percentage of relief as found in the Household Income Table.
Medical Expenses Instructions
Part I, Line 10 or Part II, Line 7
“Medical expenses paid” includes all 2014 medical expenses incurred for and paid by the applicant, spouse, or owner-occupant.
In general, medical expenses include any payments you made that would qualify for the income tax medical expenses deduction
on Federal Form 1040, Schedule A, line 1; except payments for the treatment of a dependent who is not an owner-occupant of
the homestead. Include all amounts that were paid during 2014, regardless of when the care was received. If your insurance
company paid the service provider directly for part of your expenses, and you paid only the amount that remained, include
ONLY the amount you paid. Do not include amounts paid on your behalf directly to the service provider by any other person
or governmental unit. IRS Publication 502 contains more information on medical and dental expenses.
Reimbursements.
Do not include any amounts you paid that have been or will be reimbursed by insurance.
Doctors, Dentists, Hospitals.
Include amounts paid for medical services such as:
1. Payments to doctors, dentists, osteopaths, nurses, chiropractors, and other licensed medical practitioners;
2. Payments to hospitals or licensed nursing care facilities; and
3. Payments for purchases of medical equipment, crutches, hearing aids, eyeglasses, contact lenses, dentures, etc.
Do not include funeral, burial, or cremation costs.
Prescription Medicines.
Include payments for prescription medicines and insulin. Prescription medicines are only those
drugs and medicines that cannot be purchased without a prescription.
Do not include any medicine that can be purchased over-the-counter without a prescription, whether or not they have been
prescribed by a doctor. For example, aspirin, vitamins, and cough drops are not prescription medicines.
Health Insurance Premiums.
Include insurance premiums paid for medical insurance for the applicant, spouse, or
owner-occupant. Medical insurance includes Medicare Part B, Medicare Supplemental, Part D Medicare prescription drug
coverage, or insurance for licensed nursing care. Part B Medicare withheld from Social Security payments should be included
as insurance premiums paid.
Do not include:
Medicare Part A deductions withheld from wages; self-employed health insurance that reduced total
income; the medical payments portion of a car insurance policy; an accident or health insurance policy where the benefits
do not specifically cover medical care; life insurance or income protection policies; employer-sponsored health insurance
plans; and flexible spending accounts. These are not deductible medical insurance premiums.
Worksheet A — Part I
Note:
Retain a copy for your records.
Line A, Net Business Income Including Rental, or Farm Income, or (Loss).
Report your 2014 net income. For
information on computing the income, refer to the following federal schedules and instructions:
1. For business income, see Schedule C, Federal Form 1040, or Schedule C-EZ, Federal Form 1040;
2. For income from rental real estate, royalties, partnerships, S corporations, trusts, REMICs, etc., see Schedule E,
Federal Form 1040; and
3. For farm income, see Schedule F, Federal Form 1040.
Line B, Capital Gains or (Loss).
Include all income or loss resulting from the sale of stock, bonds, or real estate from
Federal Forms 1099-B, 1099-S, 1099-R, 1099-DIV, or equivalents. See Schedule D, Federal Form 1040.
Line C, Other Gains or (Loss).
Report all other gains or losses on tangible or intangible property not included on line A
or line B. See Federal Form 4797.
Line D, Unemployment Compensation.
Include all unemployment compensation received for 2014 from Box 1,
Federal Form 1099-G.
Line E, Any Other Income or (Adjustments Reducing Income).
Report all other income (from Federal Form 1099-MISC
or other Forms 1099), taxable state income tax refunds reported on Federal Form 1099-G, and all alimony received. Report
any adjustments reducing income such as moving expenses, IRA deductions, student loan interest, tuition and fees, self-
employment tax and self-employment health insurance, SEP, SIMPLE, and other qualified retirement plans, and alimony paid.
Refer to the instructions for Federal Form 1040. Health expenses and health insurance premiums other than self-employment
health insurance should be entered on line 10a.
Subtract the calculated adjustments from the calculated “other income” and enter the net income or loss on line E.
LINE F, Penalty on Early Withdrawal of Savings.
Report your total amount of penalties for early withdrawal of savings
from Box 2, Federal Form 1099-INT.
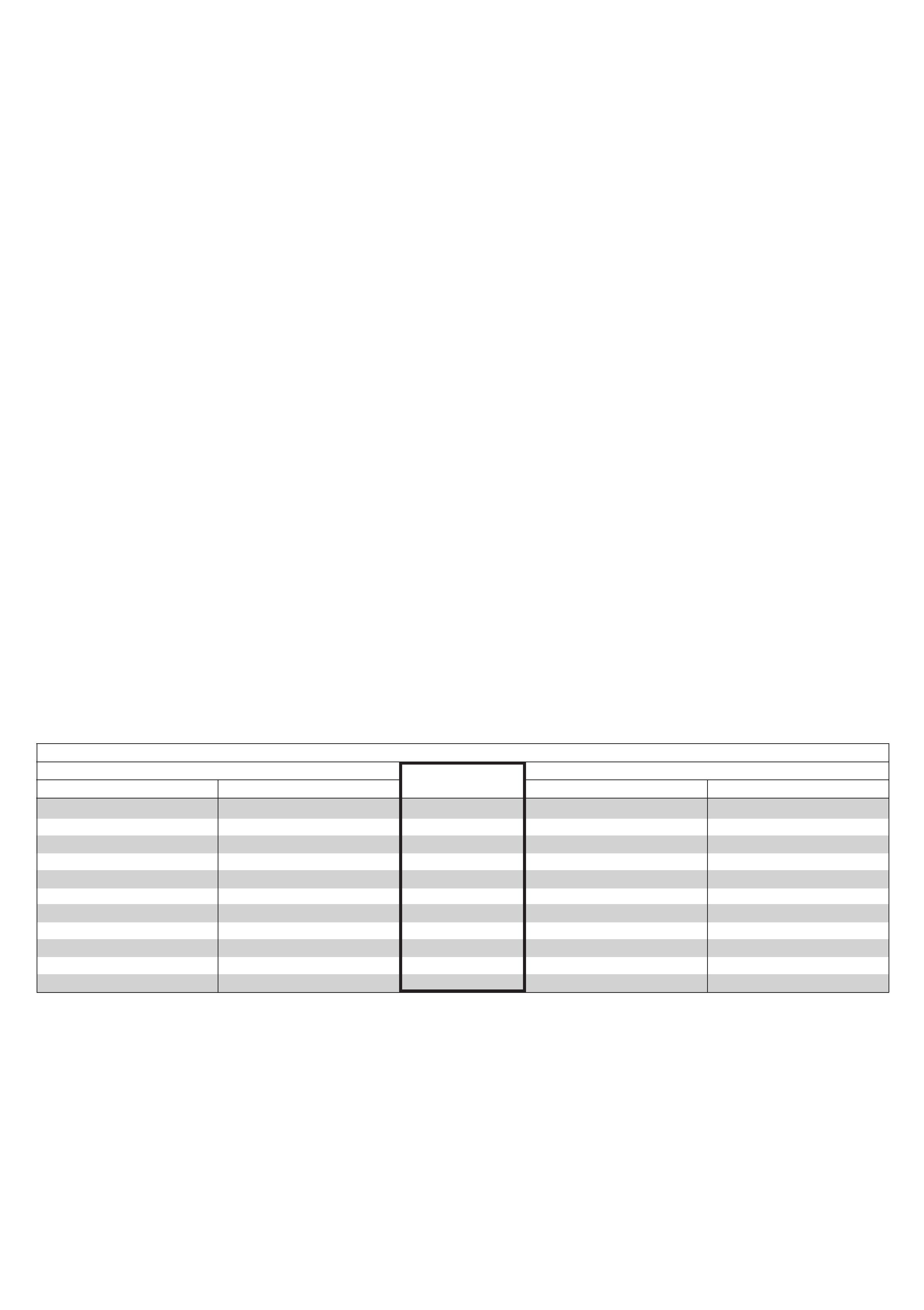
Household Income Table
Over Age 65
Single Married Single Married
Disabled Veterans & Disabled Individuals
Percentage
of Relief
$ 0 — $27,300.99 $ 0 — $32,000.99 100% $ 0 — $30,700.99 $ 0 — $35,200.99
27,301 — 28,700.99 32,001 — 33,800.99 90% 30,701 — 32,200.99 35,201 — 36,900.99
28,701 — 30,100.99 33,801 — 35,500.99 80% 32,201 — 33,600.99 36,901 — 38,700.99
30,101 — 31,500.99 35,501 — 37,200.99 70% 33,601 — 35,000.99 38,701 — 40,400.99
31,501 — 33,000.99 37,201 — 39,000.99 60% 35,001 — 36,400.99 40,401 — 42,100.99
33,001 — 34,400.99 39,001 — 40,700.99 50% 36,401 — 37,800.99 42,101 — 43,800.99
34,401 — 35,800.99 40,701 — 42,400.99 40% 37,801 — 39,300.99 43,801 — 45,600.99
35,801 — 37,200.99 42,401 — 44,100.99 30% 39,301 — 40,700.99 45,601 — 47,300.99
37,201 — 38,700.99 44,101 — 45,900.99 20% 40,701 — 42,100.99 47,301 — 49,000.99
38,701 — 40,100.99 45,901 — 47,600.99 10% 42,101 — 43,500.99 49,001 — 50,700.99
40,101 and over 47,601 and over 0% 43,501 and over 50,701 and over
For more information, see revenue.nebraska.gov/PAD, or call 888-475-5101 or 402-471-6185.


