
Fillable Printable Attendant Care Company
Fillable Printable Attendant Care Company
Attendant Care Company
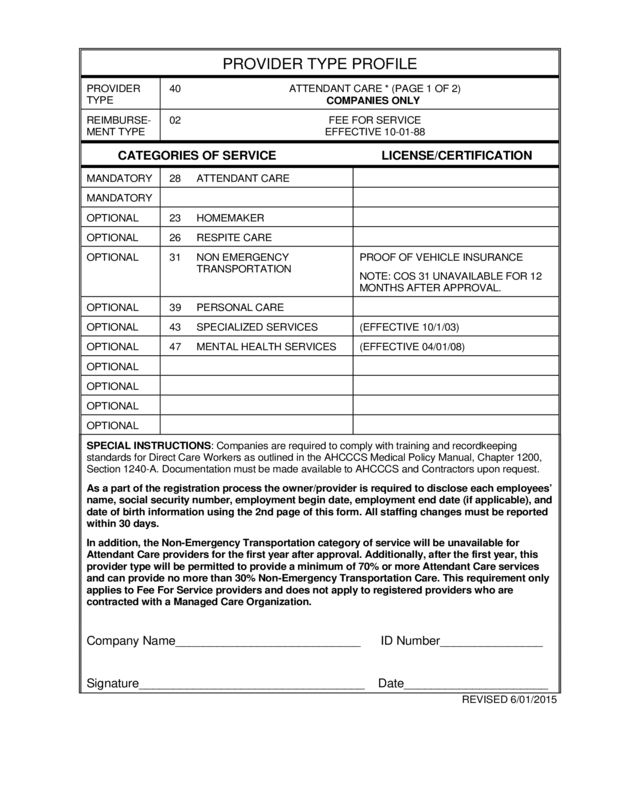
PROVIDER TYPE PROFILE
PROVIDER
TYPE
40 ATTENDANT CARE * (PAGE 1 OF 2)
COMPANIES ONLY
REIMBURSE-
MENT TYPE
02 FEE FOR SERVICE
EFFECTIVE 10-01-88
CATEGORIES OF SERVICE LICENSE/CERTIFICATION
MANDATORY 28 ATTENDANT CARE
MANDATORY
OPTIONAL 23 HOMEMAKER
OPTIONAL 26 RESPITE CARE
OPTIONAL 31 NON EMERGENCY
TRANSPORTATION
PROOF OF VEHICLE INSURANCE
NOTE: COS 31 UNAVAILABLE FOR 12
MONTHS AFTER APPROVAL.
OPTIONAL 39 PERSONAL CARE
OPTIONAL 43 SPECIALIZED SERVICES (EFFECTIVE 10/1/03)
OPTIONAL 47 MENTAL HEALTH SERVICES (EFFECTIVE 04/01/08)
OPTIONAL
OPTIONAL
OPTIONAL
OPTIONAL
SPECIAL INSTRUCTIONS: Companies are required to comply with training and recordkeeping
standards for Direct Care Workers as outlined in the AHCCCS Medical Policy Manual, Chapter 1200,
Section 1240-A. Documentation must be made available to AHCCCS and Contractors upon request.
As a part of the registration process the owner/provider is required to disclose each employees’
name, social security number, employ ment begin date, employ ment end date (if applicable), and
date of birth information using the 2nd page of this form. All staffing changes must be reported
within 30 days.
In addition, the Non-Emergency Transportation category of serv ice will be unavailable for
Attendant Care providers for the first y ear after approv al. Additionally , after the first y ear, this
provider ty pe will be permitted to provide a minimum of 70% or more Attendant Care serv ices
and can provide no more than 30% Non-Emergency Transportation Care. This requirement only
applies to Fee For Service providers and does not apply to registered providers who are
contracted with a Managed Care Organization.
Company Name___________________________ ID Number_______________
Signature_________________________________ Date_____________________
REVISED 6/01/2015
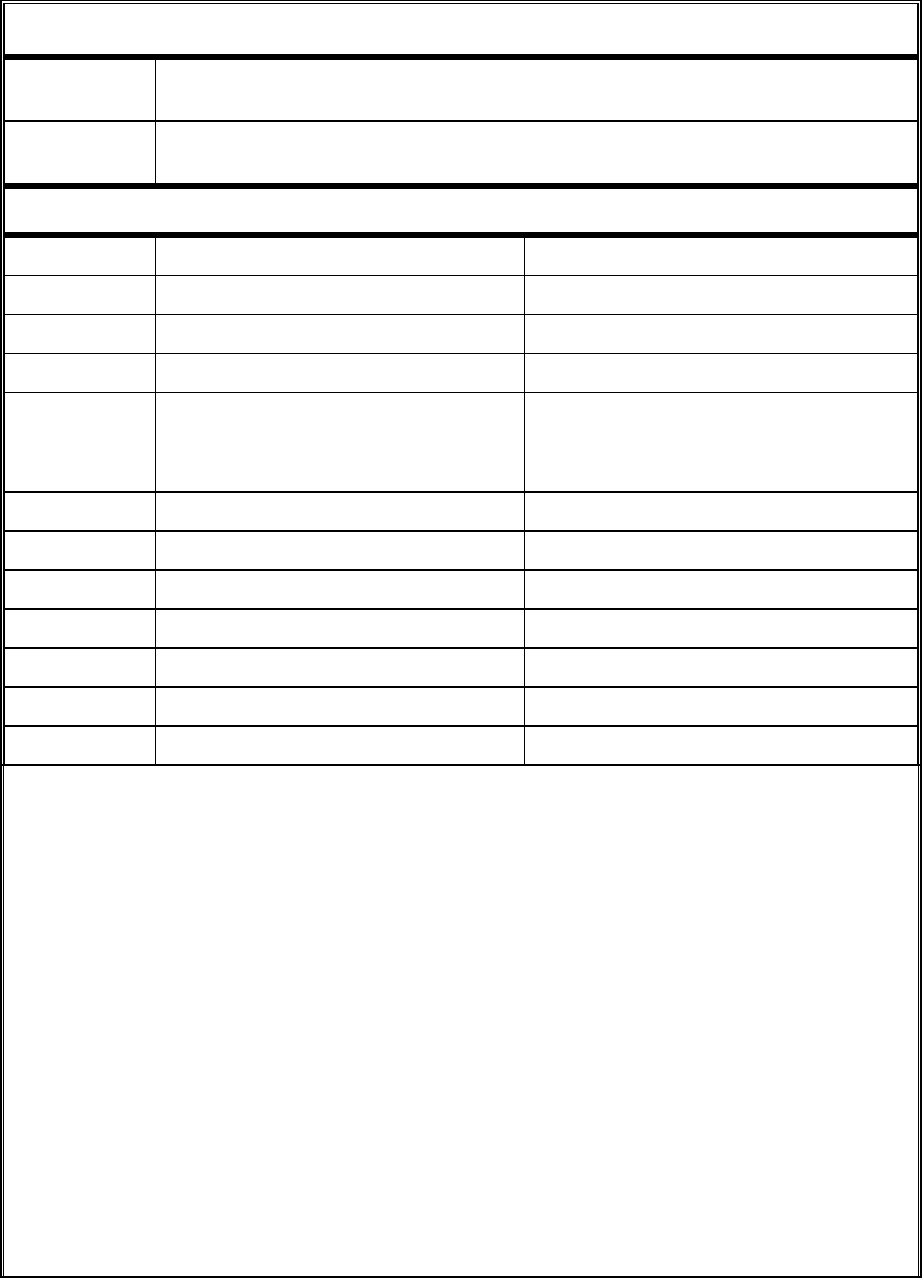
PROVIDER TYPE PROFILE
PROVIDER
TYPE
40
ATTENDANT CARE * (PAGE 2 OF 2)
COMPANIES ONLY
REIMBURSE-
MENT TYPE
02
FEE FOR SERVICE
EFFECTIVE 10/01/1988
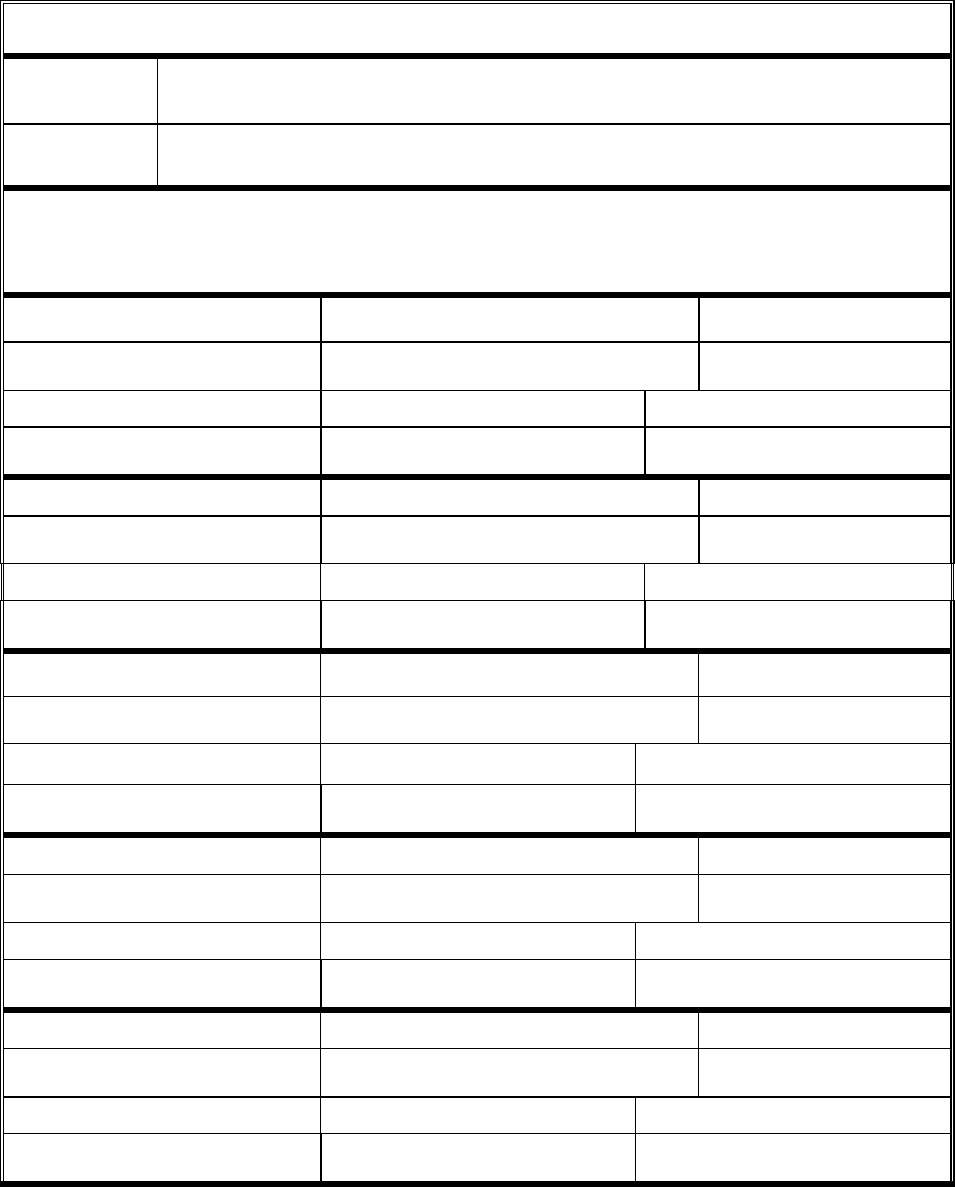
List of Employees
(ALL FIELDS ARE MANDATORY)
Last Name:
First Name, Middle Initial:
SSN:
Employment Begin Date:
Employment End Date:
Date of Birth: (MM/DD/YYYY)
Last Name:
First Name, Middle Initial:
SSN:
Employment Begin Date:
Employment End Date:
Date of Birth: (MM/DD/YYYY)
Last Name:
First Name, Middle Initial:
SSN:
Employment Begin Date:
Employment End Date:
Date of Birth: (MM/DD/YYYY)
Last Name:
First Name, Middle Initial:
SSN:
Employment Begin Date:
Employment End Date:
Date of Birth: (MM/DD/YYYY)
Last Name:
First Name, Middle Initial:
SSN:
Employment Begin Date:
Employment End Date:
Date of Birth: (MM/DD/YYYY)
Copy if additional pages are needed. REVISED 1/9/2015
This information is required in accordance with 42 CFR 455 Subparts B and E and State Medicaid Director Letters
08-003 & 09-001.
Reset


